Fetal alcohol spectrum disorders (FASDs) is an umbrella term used to describe the range of effects that can occur in an individual with prenatal alcohol exposure. These effects can have lifelong implications including physical, mental, behavior, and/or learning issues.
The exact number of children who have an FASD is difficult to determine. Some experts estimate that approximately 40,000 babies may be born with an FASD in the United States each year. Based on studies of the Centers for Disease Control and Prevention and others, it is estimated that in the United States, somewhere between 800 and 8,000 babies could be born each year with fetal alcohol syndrome (FAS).
Conditions on the FASD Spectrum
The term FASD encompasses a number of conditions:
Fetal Alcohol Syndrome (FAS)
 FAS is on the most severe end of the FASD spectrum. It describes people with the greatest alcohol effects, causing signs and symptoms so distinct that the diagnosis is based on special measurements and findings in each of the 3 following areas:
FAS is on the most severe end of the FASD spectrum. It describes people with the greatest alcohol effects, causing signs and symptoms so distinct that the diagnosis is based on special measurements and findings in each of the 3 following areas:
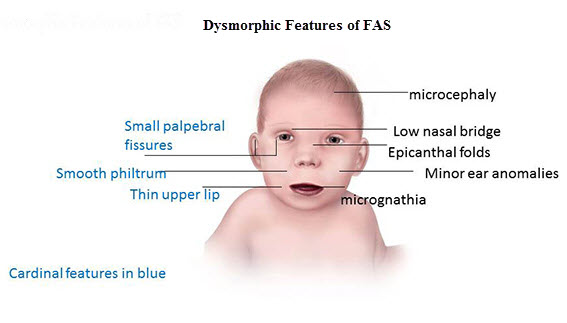
Three specific facial abnormalities: smooth philtrum (the area between nose and upper lip), thin upper lip, small palpebral fissures (the horizontal eye openings)
Growth deficit (lower than average height, weight or both)
Central nervous system (CNS) abnormalities (structural, neurologic, functional, or a combination of these)
Partial fetal Alcohol Syndrome (pFAS)
When a person does not meet the full diagnostic criteria for FAS but has a history of prenatal alcohol exposure and some of the facial abnormalities, as well as a growth problem or CNS abnormalities that person is considered to have partial FAS (pFAS).
Alcohol-Related Neurodevelopmental Disorder (ARND)
People with ARND do not have abnormal facial features or growth problems, but do have problems with how their brain and nervous system were formed as well as how they function. These individuals may have:
In particular, a 2011 federally convened committee that reviewed the science noted that these children are most likely to have problems with neurocognitive development, adaptive functioning, and or behavior regulation.
Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure (ND-PAE)
In addition to confirmed prenatal alcohol exposure, these individuals have impairment of neurocognition, self-regulation, and adaptive functioning. ND-PAE combines deficits is these three areas in conjunction with the following:
Evidence of prenatal alcohol exposure
Childhood onset of symptoms
Significant distress or impairment in social, academic, occupational, or other important area of function
Alcohol-Related Birth Defects (ARBD)
People with ARBD have problems with how some of their organs were formed and or how they function, including:
These individuals also may have one of the other FASDs.
Cause
FASDs can happen only when a pregnant woman consumes alcohol. The alcohol crosses the placenta and enters the baby's blood where it can damage the developing brain and other organs leading to an FASD. FASDs are 100% preventable if a woman does not drink alcohol during pregnancy.
Diagnosis
It is difficult to diagnosis FASDs, because there is no single or simple test that can cover the broad range of FASD signs and symptoms. Certain physical findings, developmental problems, behavioral concerns, or school failure should trigger the parents and or the pediatric medical home provider or other pediatric developmental specialist to consider FASDs as potential diagnoses, especially in the context of exposure to prenatal alcohol. A known history of alcohol consumption during the pregnancy aids in diagnosis but is not required for diagnosis of an FASD.
Children with an FASD can have brain abnormalities that lead to problems in day-to-day functioning despite having a normal IQ, so a comprehensive evaluation is indicated. All children with involvement in foster care or adoption processes―especially international adoptions―should always be evaluated for a possible FASD.
Treatment
No one treatment is right for every child, as FASD and its constellation of symptoms differ from one child to another. FASDs need a medical home to provide, coordinate, and facilitate all the necessary medical, behavioral, social, and educational services.
Many types of available treatments include but are not limited to:
Developmental services
Educational interventions
Behavior modification
Parent training
Social skills training
Medications and other medical therapies
Transition planning
Advocacy in school and the workplace
Referral for community support services
Coordination across the specialists, partners, and needed supports
Primary care in a high quality medical home setting with care integration
Treatment plans should be adaptable to the child's and family's needs, plus include close monitoring and follow-up.
Outlook for Children with FASDs
FASDs last a lifetime. There is no cure for FASDs, but identifying children with FASDs as early as possible can help them reach their potential. Research has shown that early identification and enrollment in treatment can significantly improve an affected child's development and life.
Additional Resources